PUV is a common congenital urological problem in male child.
PUV is a common congenital urological problem in male child.
Posterior urethral obstruction was first classified by H. H. Young in 1919.
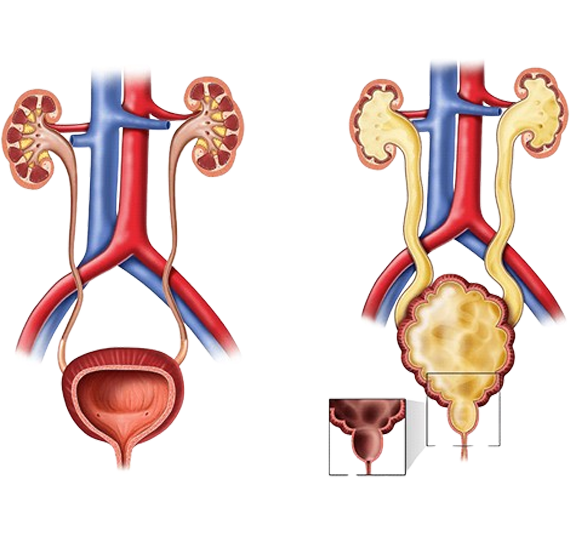
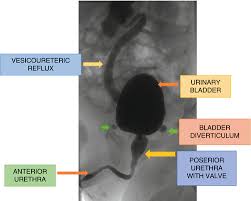
Pregnancy: PUV can be diagnosed before birth, or even at birth when the ultrasound during pregnancy shows that the male baby has a hydronephrosis, hydro-ureteronephrosis, thickened bladder wall and posterior urethra, oligohydramnios (AFI).
Birth: presentation immediately after birth can be a painful or forceful micturition, dribbling, poor stream of urine, retention of urine scrotal swelling.
Babies with oligohydramnios due to the urinary obstruction may have respiratory distress. It is an emergency. Baby may need Oxygen support, fluid and electrolyte therapy and urinary diversion.This is followed by definitive surgery when stable.
Later in Chilhood : Poor stream of urine, urinary tract infection, diurnal enuresis, abdominal distension, scrotal swelling in severe cases.
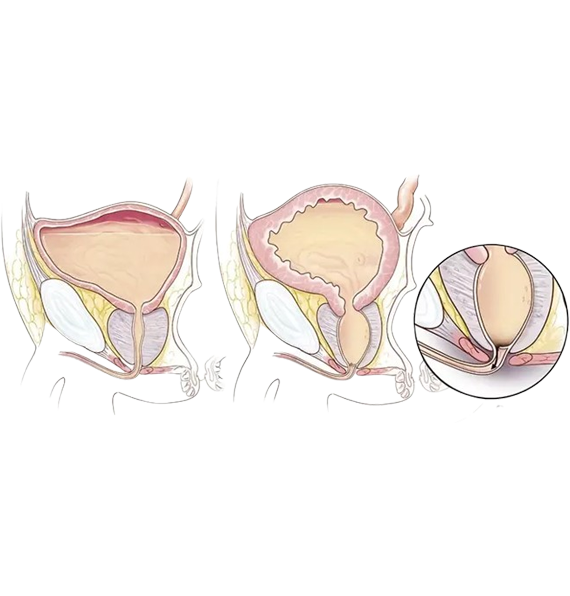
Postvesicular obstruction due to urethral valves.
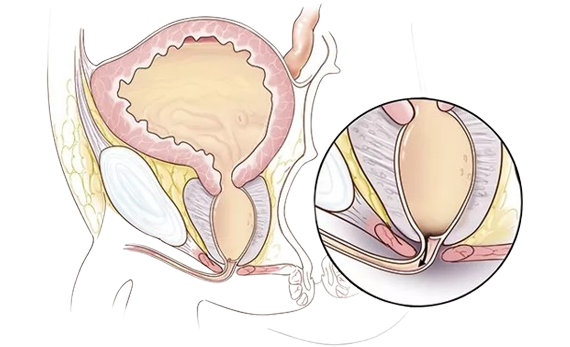
THE STANDARD TREATMENT IS PRIMARY (TRANSURETHRAL) ABLATION OF THE VALVES.
It is done by CYSTO-URETHROSCOPY using Pediatric Cystoscope or Resectoscope with
LASER OR ELECROCUATERY with fine bugbee electrodes (please see our operative videos).
If suspected during Pregnancy (antenatally), a consultation with paediatric urologist maybe indicated to evaluate the risk and consider treatment options.
There are three specific endoscopic treatments of posterior urethral valves:[citation needed]
Following surgery, the follow-up in patients with posterior urethral valve syndrome is long term, and often requires a multidisciplinary effort between paediatric urologists, paediatric nephrologists, pulmonologists, neonatologists, radiologists and the family of the patient.
Care must be taken to promote proper bladder compliance and renal function, as well as to monitor and treat the significant lung underdevelopment that can accompany the disorder. Definitive treatment may also be indicated for the vesico-ureteral reflux.

Best diagnosis and good behaviour. We are taking treatment since 1 year. My child is now good . Thank you doc.

Our baby was suffering from urology problem since birth. Perfectly diagnosed and treated at uro kids clinic by dr aadil sir. The behaviour of doctor and team was extremely cooperative. Thnx so much.

Best pedratic urology Thank u so much Adil foorqui sir.... Our baby was suffering from chronic UTI and urinary bladder problem... We have tried so many centres. But after long time we r satisfied with Dr. Aadil Farooq And now our baby is doing well and good.. Thanks once again sir.

Very experienced Doctor for kids urology related issues. Helped one of my friends baby with kidney functioning problem since birth and provided exceptional services and care during entire process. Guided them to the right direction which improved kid's condition a lot.

I highly recommend Dr. Aadil Farooq Sir for pediatric urology.our low birth baby was successfully operated & treated by sir. Thanks

Best doctor I have ever seen in my life so kind. I want say thank you for your best services. God bless you and your family ❤

Great response in behaviour at uro kids clinic Comparative team. Perfect surgery . Now my child is healthy. Thanks to Dr. Aadil Farooq and team

Dr. aadil Farooq excellent doctor, he is very caring, soft spoken and great humanitarian. Outstanding Pediatric urologist. Operated our son...happy family and child.

Good behavior,great response,May almighty showers is blessings on you

Dr. with humanity and good knowledge. Like his way of dealing patients.

He is the best paediatric urologist all over Rajasthan in present time.

Great Pediatrics urologists of Rajasthan.Very excellent skills and cooperative behaviour.

One of the best paediatric urologist in jaipur. Very kind in nature, knowledgable and gentle with patients. Must visit if u r searching paediatric surgeon in rajasthan

डॉ आदिल बहुत प्रतिभाशाली हैं और वे हमेशा कम से कम जांच के साथ, कम से कम दवा के साथ रोगी का इलाज करना चाहते हैं।

He is a very good pediatric urologist in Jaipur. Best of the business. He is very experienced and and very price effective Dr. If you get any urology related problems under 18 years so can contact him. A very brilliant doctor he is.

Dr.Aadil Farooq is one of the Top Superspecialist In Pediatrics Urologist and surgeon available in Rajasthan.... Visit Him For Better Care