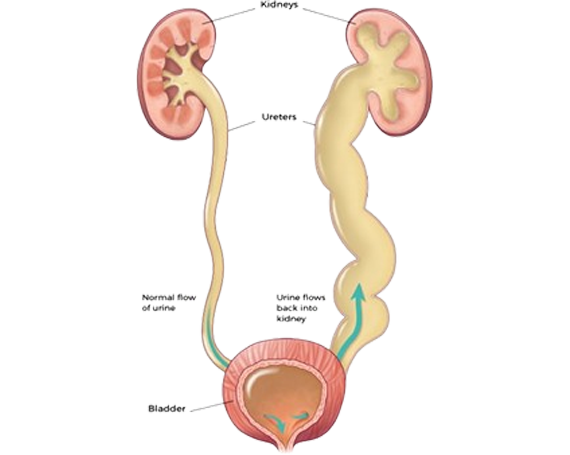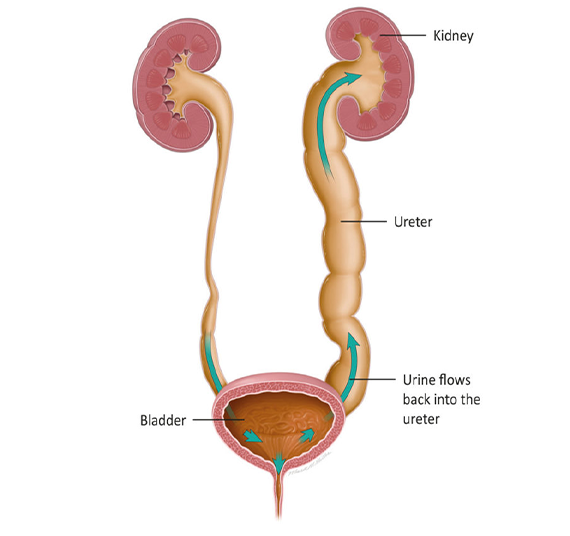
The kidneys produce urine, which travels down tubes called the ureters. The ureters empty into the bladder where urine is stored. During urination, the bladder contracts & urethral sphincter relaxes.
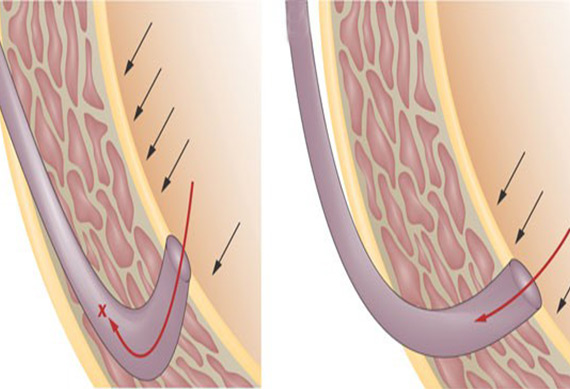
Vesicoureteral reflux (VUR) occurs when urine in the bladder flows back into one or both ureters and often back into the kidneys. This may occur because of the position of the ureter in the bladder wall.
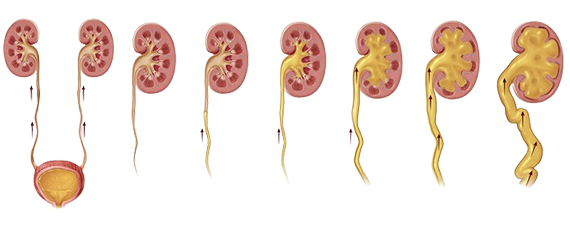
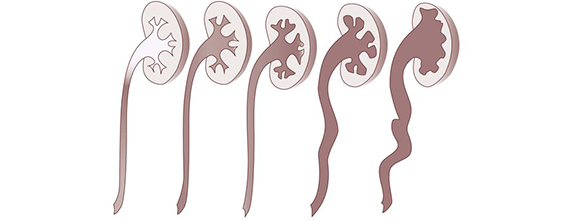
VUR is graded according to severity from grade 1 (mild) to grade 5 (severe).
The level of severity is determined by urine flow and the extent of the associated dilation.
Testing and diagnosis
Voiding cystourethrogram (VCUG) is used to confirm the diagnosis of VUR. The VCUG takes 15 to 20 minutes.